If nothing else, the current Corona virus pandemic has focussed us on the need for data to assess risk and to inform policy. However, it is one thing to produce data and another to weigh it’s validity and to interpret what the underlying message is. It is with this in mind that we must be very careful how we judge how well our decision makers have performed in the current crisis. The real test is that of a historian who will ask whether any other course of action was viable given the background ‘noise’ and ‘chatter’ and contradictory expert advice.
Having said that there was one set of data that caught my eye as it touched on not one but two of my previous essays (see below). In an article in The Times, Kat Lay had reported that the doctors in the NHS were concerned that patients were holding off attending A&E because they were afraid of catching the Corona virus. For English hospitals, the number of attendees had fallen by 57%, comparing April 2020 with April 2019. In whole numbers, that means a reduction of 1.2 million visits, month on month. “Dr Nick Scriven, immediate past president of the Society for Acute Medicine, said the drop in A&E attendances was “a significant concern” and people’s conditions may have worsened as a result.
“This is a ticking timebomb in itself and it will be exacerbated by a myriad of other pressures in the coming weeks,” he said.”(The Times 14/05/20)
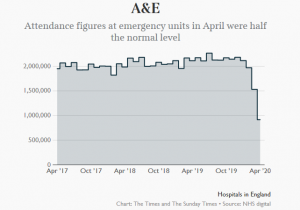 Of course there are some obvious reasons for the decline in numbers mentioned in the article and referenced on the graph opposite. Working from home means that there is far less traffic on the roads and partly for this reason there were 27,000 fewer ambulance calls y-on-y. What is missing from the article and the medical references, is voiced in the comments attached to the article and was the subject of my earlier essays (see below). It is the elephant in the room. Let’s take a couple of comments that give a flavour of the frustration of readers with the journalist, for not asking the obvious questions.
Of course there are some obvious reasons for the decline in numbers mentioned in the article and referenced on the graph opposite. Working from home means that there is far less traffic on the roads and partly for this reason there were 27,000 fewer ambulance calls y-on-y. What is missing from the article and the medical references, is voiced in the comments attached to the article and was the subject of my earlier essays (see below). It is the elephant in the room. Let’s take a couple of comments that give a flavour of the frustration of readers with the journalist, for not asking the obvious questions.
Willie Deadwilder: Surely this is to be expected. Fewer drunks on the streets means fewer admissions to A&E plus fewer people at work means fewer workplace accidents. It’s not rocket science.
Lenny:Of course you are right. Why can’t our dozy journalists do some basic research or ask the right questions to A&E staff? It does not fit with the prevailing narrative of doom and gloom.
Paramaniac: I work in the Ambulance Service and all I can say is thank you lord, thank you so much for giving us a small break in the mind numbing incessant c**p we normally go to.
I realise it won’t be for long and once C19 is over we’ll be back to doing the incessant mind numbing c**p we do in the Ambulance Service but thanks for while it lasted.
What wasn’t discussed in the article was the effect of those who either attend A&E because it is free or, they can’t be bothered to go to their GP and those who attend because of anti social behaviour. Of course, there are a number of people who don’t attend, who should attend. There are those who feel that they shouldn’t bother the Health Service at this time and stoically suffer on when they should seek help. There are those who are afraid of catching the virus, whose condition will deteriorate and they will be one of the ambulance calls that will become an emergency. What we don’t see in this article is the reason for the paramedics prayer of thanks in the Comments.
How does this article and it’s omissions connect with my two essays on the subject. The first one, entitled Minister for Health (03/09/18 see below) described my reaction to the unveiling of a new health plan entitled Sláintecare. I suggested that a plan cannot be a plan without costings otherwise it is merely the Ministers aspiration. I went further to suggest that there appeared to be a dearth of management information that would serve as a platform for making plans. For example, at the time there was a lot of heat being generated about people on trolleys in A&E. However, there seemed to be very little light in the way of in depth verifiable data on the subject. We just about knew the number of people involved but even this was a source of dispute between the HSE and A&E Unions but beyond that, very little. My second article Addendum to the ‘Minister of Health Article (01/03/20 see below) followed up on the first one by commenting on the statistic that in 2018 the HSE conducted a survey of 293,976 hospital discharges and found that 33,929 (11.5%) patients were discharged the same day and 55,510 (18.8%) were discharged within 24 hours. There seemed to be a curious lack of interest as to why this was the case. The lack of Junior Consultants at night was one guess that was hazarded but there appeared to be no real effort or, ambition, to discover how many of those discharged within 24 hours should have been there in the first place.
We can sense a theme running through these observations with similar characteristics. First of all and most obviously there seems to be a dearth of detailed information in relation to Health issues. The issue of under resourcing A&E has been a long running story for a number of years but we only see a large scale survey being made in 2018. I have yet to see a comprehensive breakdown on these numbers that would be the basis for solving the problem. Secondly, part of the reason for lack of any cohesive logical response is the quality of reporting. In the case of the current Times report perhaps Kay Lay should take Lenny’s advice in the Comments section and do a follow up article based on an interview with Paramaniac or, one of his/her colleagues. Thirdly, as mentioned in my first essay, there is no responsibility for value for taxpayers money in the Health service. The Children’s Hospital is a prime example of this. For one of the most expensive capital projects in the health service there was an incompetent political and managerial oversight of the project. There has to be far more transparency and ownership of all parts of the health service. In my essay I suggested that there should be an independent internal audit section that would publish its findings on a regular basis and make clear who is responsible in cases of failure. Fourthly, an outsiders view of the Health Service is that it is being run mainly for the benefit of employees and not the patients. I hasten to add that frontline staff are heroically trying to perform miracles in an environment that seems to be in constant crises. However, when the budget is increased there never seems to be any question of making efficiencies, for example reducing administrative staff in favour of front line and medical support staff. Instead, what we see is a form of internecine warfare to make sure that everyone in the industry gets their share. Perhaps that is too harsh a criticism at a time where frontline staff are risking their lives but I think on reflection there is a feeling that they are, ‘Lions led by donkeys’. Lastly, the poor old politicians must share in the ‘Donkey’ category. They have distanced themselves from the management of the service and are reluctant to get bogged down in any attempt to make it more efficient and up to date. The inmates run the asylum and react very strongly to any attempt to change the status quo.
Having said that, there is much to treasure and we see, on a daily basis, the commitment and self sacrifice that health workers are prepared to undergo in their service to others. It is the system and management, both political and operational, that need to change to match this level of service.
References
The Times, 14/05/20, Kat Lay, Coronavirus: A&E visits plunge to lowest on record,